


Michigan PH Reports on 2 H5N1 cases - IRAT Update - CO Cats - Lessons Keep Coming to Further Paint the Big Picture
I summarize weekly events of the past week and opportunities arising as a result of a rapidly evolving H5N1 2.3.4.4b cattle spillover picture

In last weekend’s (August 3rd) post I made a statement I want to bring back this week to reemphasize:
The key factor we can often overlook or minimize is the date of sampling (farm visit) versus the date of estimated initiation of clinical illness (if observed). Antigen (PCR) results are not like serology results - they can be very unstable even over 24 hours as infections progresses on dynamic surfaces like nasal mucosa. Positive nasal swab results do not remain reliably positive over long periods.
Thursday the New England Journal of Medicine published a letter from Michigan state public health officials describing results from their investigations of 2 dairy herd employee-related H5N1 zoonotic infections in their state on separate farms:
This letter did an excellent job of documenting the chain of events in each case, which were quite different in many respects. Case 1 was strictly an H5N1-origin conjunctivitis swab detection, resulting from a milk splash to a worker on a confirmed infected farm. A simultaneously collected nasopharyngeal swab was negative, indicating no respiratory involvement. The conjunctival sample was later fully sequenced at CDC and deposited as an H5N1 2.3.4.4b B3.13 influenza virus: A/Michigan/90/2024. A follow-up swab taken one week later was negative.
Case 2 was a much more epidemiologically interesting. The worker reported upper respiratory illness prior to later confirmed diagnosis in the dairy herd; however, the worker’s diagnosis was delayed due to lack of influenza PCR sampling initially at an urgent care clinic. The NEJM letter provides a good write-up of the chain of events: however, I have reproduced them on a daily timeline to simplify understanding the chain of events both at the farm and with the employee and his health care providers:
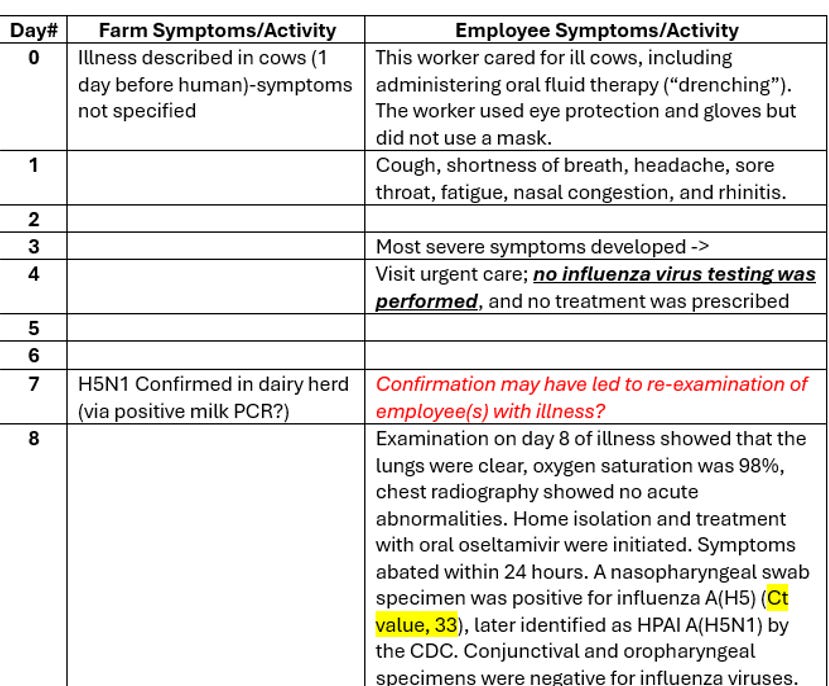
According to the letter, the cows showed “symptoms of illness” 1 day prior to the worker self-recognizing upper respiratory symptoms. This is not a veterinary paper, so we do not have more details on those symptoms, i.e. whether that included mastitis, respiratory symptoms, other, or some combination. The write-up does state that the employee was involved in drenching cattle, implying close contact with oral fluids and nasal discharge; no references were made to any direct or indirect contact he may have had with milk.
At 3-4 days he visited an urgent care clinic, presumptively for respiratory symptoms, but was not prescribed medication, tested for any respiratory pathogens, nor prescribed any treatments.
H5N1 influenza was confirmed in the dairy herd 7 days after “showing signs of illness”. Apparently, the worker chose to present at a clinic for testing (including PCR and full respiratory assessment), based on his history of and ongoing respiratory illness and the H5N1 herd diagnosis. His nasopharyngeal swab contained enough residual viral RNA for detection (CT=33), although oropharyngeal and conjunctival swabs were negative. CDC was partially successful in characterizing the virus as H5N1, but unable to generate full sequence or isolate live virus.
This public health epidemiology write-up holds important information for both human and animal health experts regarding the importance of timing in case history and sample collections. If we assume intranasal spread of the virus from cows to the worker as an indicator of viral spread from the dairy herd, then our current dairy herd case definition(s) are not capturing early phases of infection in at least some herd infections. This herd showed unspecified signs of illness 7 days prior to H5N1 confirmed diagnosis, and that illness led to likely viral spread to a human in close contact with the heads of ill animals. This means that respiratory swab diagnostics in symptomatic cows concurrently with symptomatic workers might have yielded positive results in both the cows and the worker earlier in the courses of infections.
The dairy side of this One Health challenge still has a belated opportunity for case diagnosis due to lactating cows that develop mastitis from H5N1 infection, leading to milk testing. However, on the human side, diagnosis depends on prompt antigenic/PCR testing while antigen remains in the oronasal / conjunctival area. If workers don’t report URI’s or emergency care fails to test at the time of acute illness, the opportunity is lost to capture virus for analysis. Waiting until the herd is diagnosed to prevail upon workers to undergo swabbing becomes a low yield proposition, because in all likelihood acute infections have passed in exposed workers. In this case the worker was ill enough to replicate virus long enough for remnants (CT=33) to remain. Additionally, the herd was diagnosed relatively quickly after first signs of clinical illness, shortening the time to when the 2nd swabbing of the worker took place thanks to public health awareness of H5N1 herd infection.
Returning to my original point from last week’s blog, prompt testing is so critical for more powerful PCR results and opportunities for viral isolation and complete genomic sequencing. A complete sequence is the ultimate goal for each positive diagnosis in both cattle and people; that information provides our molecular epidemiologists and biologists with the raw information needed for monitoring ongoing threats as the virus continues to evolve.
Documented human cases of H5N1 in dairy workers should not be rare, given the number of infected herds and numerous anecdotal reports of sick workers on dairy farms as cows become ill. The relatively high number of reported cases in poultry depopulation workers in Colorado further supports susceptibility to virus transmissibility to people lacking fairly robust PPE. That data also supports that prompt testing at the onset of clinical illness aids in successful detection.
None of this information in the NEJM letter is exceptionally revelatory, and it certainly doesn’t provide an easy solution to improve voluntary compliance with prompt human or cattle sampling. I personally believe that economical lateral flow-like antigen testing kits for H5 (or even existing Matrix gene kits) could be used in the field to screen for influenza in both people and cattle on or near the farm. There are certainly legal pitfalls with utilizing that technology; however, we must somehow make testing more frequent, easier and immediate through widespread on-farm screening. Assays not run or run too late are inherently 0% sensitive. Our H5 PCR test structure for dairy workers approaches 0% sensitivity for that reason. The tests are technically fine but applied very poorly because we lack delivery processes to put the tests in the right place at the right time.
For cattle herds, the question is a bit more complex. I’d argue that we’re getting a good diagnosis (good sensitivity) in the lactating dairy herds that we test, but we’re only testing dairy herds that develop mastitis. We have failed to do even basic serological studies to determine if our practical case definition (mastitis in lactating cows) is broad enough to capture all H5N1 infections in cattle in general.
Furthermore, our existing diagnostics are late, in that we base them mostly on clinical mastitis, a later-developing clinical sign in infected lactating dairy herds. Bulk milk sampling in lactating cows may help timeliness versus utilizing clinical mastitis; however, oronasal sampling protocols would also be useful in all classes of cattle if a good case definition for bovine respiratory/systemic influenza infection can be developed.
In another H5N1 2.3.4.4b B3.13 development, CDC released its latest pandemic risk assessment for this virus: Results of Influenza Risk Assessment Tool | Pandemic Flu | CDC. This is the first IRAT assessment that utilized ferret transmission studies from the April 2024 Texas H5N1 Texas case, but did not include later work related to the Michigan isolate (referenced above) or any of the recent CO poultry worker isolates.
Here is the conclusion regarding the current U.S. avian H5N1 for those who want to skip reading the entire report:
This report summarizes the findings of an IRAT conducted on a recent avian influenza A(H5N1) virus from a human case in Texas (A/Texas/37/2024). The score places the currently circulating avian influenza A(H5N1) virus in the category of "moderate risk" for potential future emergence and public health impact. This is similar to previous assessments of earlier avian influenza A(H5N1) viruses. The scores for this IRAT were submitted June 26, 2024, prior to additional human cases in Colorado. The report was completed expeditiously based on data as of June 26 to inform ongoing preparedness discussions.
As always, any assessment is valid for current genotypes, subject to changes as the genomic pattern changes over time. That is why ongoing surveillance and viral sequencing in both animals and people is so critical in preparedness.
Although announced a while back, Colorado reported 10 new infected herd last week discovered via bulk tank milk testing, bring their total infected herd count to 63. Bulk tank testing added 19% to their total in one week! We really are at the point where herd counts are of secondary importance. Entire states and the dairy industries within them are likely not reporting infected herds, and we have no serological evidence to justify current status in either previously infected herds or in unknown status areas. No one has a known negative status through valid testing to my knowledge. Colorado’s bulk tank testing results add one more brick to the load arguing that the full extent of this virus is badly understated.
Speaking of Colorado, be sure to check out an important LinkedIn Post by Kay Russo, a recent cofounder of RSM Consulting, LLC, and an experienced dairy and poultry veterinarian with extensive H5N1 experience. Her post highlights a new warning from the Colorado VMA to cat owners related to a flurry of 6 cat fatalities due to H5N1 influenza in that state:
(only) One of these cases was directly associated with a known infected commercial dairy facility. Two of the six cases were indoor only cats with no direct exposures to the virus. Three of the six cases were known indoor/outdoor cats that hunted mice and/or small birds as prey and also spent time indoors with their owners. Five of the six cases have presented with similar clinical signs and disease progression: an initial complaint of lethargy and inappetence, followed by progressive respiratory signs in some and fairly consistent progressive neurologic signs in most. Several of these cases were tested for rabies preceding diagnosis with H5N1 infection due to the indistinguishable presentation once neurologic signs presented. HPAI H5N1 infection should be considered in domestic felines even if all of the risk factors or clinical signs are not present. There is high abundance of virus in Colorado at this time, predominantly being detected in domestic dairy cattle in commercial dairy herds with spillover into mammals and wild birds on and near these premises. Notably the B3.13 strain of the Eurasian 2.3.4.4b clade H5N1 virus has been spreading in animals not historically attributed as reservoirs for the HPAI virus. This lineage of virus has not been detected in migratory waterfowl at this time.
One has to ask how we can effectively protect cats in NE Colorado at this time? What advice should be given to laying flock owners (and their stockholders and bankers) determining whether the “high abundance of H5N1 virus in Colorado” will continue, making repopulation of their layers inadvisable? More basically, what are the factors in NE Colorado that allowed this virus to so wickedly take off in the past few months?
Bovine H5N1 influenza is likely rapidly becoming endemic in the U.S. dairy industry, given all the unrestricted movement within both the dairy and beef industries. Both poultry and humans (and even cats) serve as “sentinels” for new infections, and retail milk samples and wastewater surveillance provide additional evidence. I’d urge that those who doubt or fear this reality should prevail upon the USDA to allow provisional serological testing for non-regulatory purposes in order to fine-tune cut-off values and determine with greater precision the degree of inroads this virus has made into cattle populations across the country.
I honestly hope I’m crying wolf over a much less serious situation. So please prove me wrong. Let’s enroll some owner-veterinarian-researcher volunteers to investigate sub-clinical early-stage (e.g. CO bulk tank positive herds) cases from beginning to resolution in the field as an outbreak unfolds. Veterinarians from previously affected herds could be consulted first to intelligently determine objectives. Include follow-up with serological sampling in both affected and healthy herd mates. Public health partners could monitor and sample workers daily as a herd becomes ill, then later recovers. If we’re going to mandate sampling, let’s use early infected herds to our advantage in studying the course of infection, resulting in documented herd epidemiological report(s) with similar information on the animal side that was found in the human Michigan public health report with which I opened the blog.
Widespread serological surveys and in-the-field real-time case monitoring and reporting (both with appropriate privacy safeguards) would be powerful tools in understanding our next steps and quantifying our risks. Do we have the honesty and courage to actually do it?
John